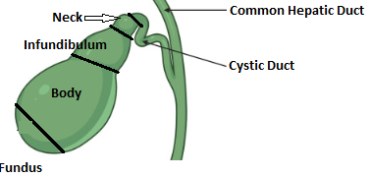
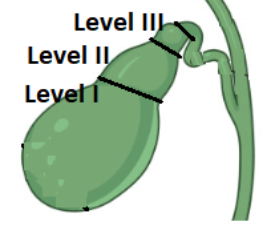
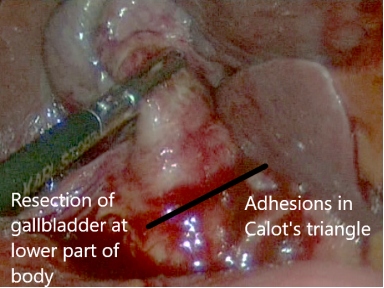
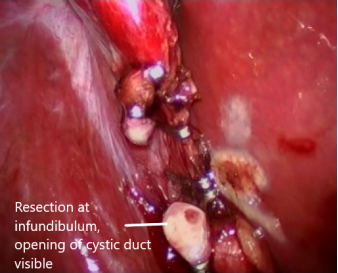
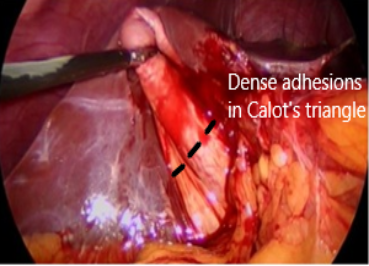
Subtotal cholecystectomy is performed in difficult gallbladder where total cholecystectomy is avoided due to risk of bile duct injury and other complications as the structures of Calot’s triangle are difficult to identify due to severe inflammation, fibrosis and dense adhesions. The remnant gallbladder can cause early and late complications such as bile leak, recurrence of stone formation and acute stump cholecystitis. The knowledge of size of remnant gallbladder in advance can help in diagnosis and decision making for handling the remnant gallbladder complications. Nigam’s Classification of Subtotal Cholecystectomy according to the Level of Resection (NCSC-LR) plays an important role in such situations and helps the treating surgeon in diagnosis and treatment of post subtotal cholecystectomy complications by knowing the level of resection (size of remnant gallbladder) as per previous operation notes.
| Published in | International Journal of Gastroenterology (Volume 9, Issue 1) |
| DOI | 10.11648/j.ijg.20250901.21 |
| Page(s) | 66-76 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Adhesions, Calot’s Triangle, Gallbladder, Level of Resection, NCSC-LR, Subtotal Cholecystectomy, Total Cholecystectomy
Type of Gallbladder diseases | Number of patients | Percentage |
|---|---|---|
Acute on chronic cholecystitis with cholelithiasis | 16 | 64% |
Empyema of gallbladder | 3 | 12% |
Gangrene of gallbladder | 6 | 24% |
Nassar Scale | Number of patients | Percentage |
|---|---|---|
Grade 1 (Early Cholecystectomy with gallbladder without adhesions) | 0 | 0% |
Grade 2 (Difficult gallbladder with simple adhesions | 0 | 0% |
Grade 3 (Challenging cholecystectomy contracted or fibrotic gallbladder with adhesions to hepatic flexure of colon or duodenum) | 15 | 60% |
Grade 4 (Dense adhesions, completely obscured gallbladder, or gangrenous gallbladder) | 10 | 40% |
Levels | Number of cases | Percentage (%) |
|---|---|---|
Level I | 2 | 8% |
Level II | 17 | 68% |
Level III | 6 | 24% |
Type of cholecystectomy | Number of patients | Percentage |
|---|---|---|
Open cholecystectomy | 11 | 44% |
Laparoscopic cholecystectomy | 14 | 56% |
Post-operative complications | Number of patients | Percentage |
|---|---|---|
Bile leak 0-5 days (through drain) | 6 | 24% |
Bile leak 6-14 days | 3 | 12% |
Bile leak 15-20 days | 3 | 12% |
Collection at gallbladder fossa | 1 | 4% |
NCSC-LR | Nigam's Classification Of Subtotal Cholecystectomy According To The Level of Resection |
CBD | Common Bile Duct |
BDI | Bile Duct Injury |
STC | Subtotal Cholecystectomy |
LC | Laparoscopic Cholecystectomy |
GB | Gallbladder |
QOL | Quality of Life |
RUQ | Right Upper Quadrant |
USG | Ultrasonogram |
CT Scan | Computed Tomography Scan |
MRCP | Magnetic Resonance Cholangiopancreatography |
HIDA Scan | Hepatobiliary Iminodiacetic Acid Scan |
ERCP | Endoscopic Retrograde Cholangiopancreatography |
| [1] | Standering S. Gray’s Anatomy: The Anatomical Basis of Clinical Practice 42nd ed. 2021. Chapter 67: p1217-1222. |
| [2] | Sanders G, Kingsnorth AN. Gallstones. BMJ. 2007; 335(7614): p295-299. |
| [3] | Malhotra SL. Epidemiological study of cholelithiasis among railroad workers in India with special reference to causation. Gut 1968; 9: p290-295. |
| [4] | R. K. Tandon, Prevalence and types of biliary stones in India. World J Gastroenterology Sept 2000; 6(Suppl 3): p4-5. |
| [5] | Sarda DK. Prevalence and management of cholelithiasis in population of Rajasthan: a clinical study. J Med Sci Clin Res. 2018; 8: p2021. |
| [6] | S Dr. Cholelithiasis: a study in clinical presentation and management. Int. J. Surg. Sci. 2020; 4: p308-310. |
| [7] | Shaffer EA. Gallstone disease: epidemiology of gallbladder stone disease. Best Pract Res Clin Gastroentero 2006; 20: p981-996. |
| [8] |
Srinivas S, Hammil CW, Strasberg SM. How to do laparoscopic subtotal fenestrating cholecystectomy. ANJ J Surg. (2021); 91(4): p740-1.
https://doi.org/10.1111/ans.16435 Epub 2020 Nov 16 |
| [9] | Mohamed E, Gianpiero G, Katie T, et al. Subtotal cholecystectomy, for difficult gallbladders – Systematic Review and Meta-analysis. JAMA Surg. 2015; 150(2): p159-168. |
| [10] | Soreide K. Gallstone disease and cancer risk: finding the bug in the system. Gastroenterology 2017; 152: p1825-8. |
| [11] | Mateja HL, Rowe DA, Tsai A, Giuseppuci P. Remnant Cholecystitis After Subtotal Cholecystectomy: A Case Report Curues. 2024 Oct 17; 16(10): e71719. |
| [12] | Teshima T, Nitta H, …. Takamori H. How to treat remnant cholecystitis after subtotal cholecystectomy: two case reports, surg case rep. 2021; 7: p109. |
| [13] | Zackria R, Lopez RA. Postcholecystectomy Syndrome. [Updated 2023 Aug 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: |
| [14] | Tokumitsu Y, Tamesa T, Shindo Y, Sakamoto K, Nagano H. Application and utility of surgical techniques for cystic plate isolation in liver surgery. Ann Gastroenterol Surg. 2022 Mar 22; 6(5): p726-732. |
| [15] | Zhou Y, Xiao L, Luo Z. Luo H, Jan Z, Wang T. Cystic plate approach in laparoscopic cholecystectomy: a consecutive retrospective analysis. Front Surg. 2024 Dec 3; 11: 1487568. Volume 11 - 2024 | |
| [16] | Griffiths EA, Hodson J, Vohra RS, Marriott P, The Choles Study Group, Ketheb T, Zino S, Nassar AHN, and West Midlands Research Collaborative. Surg. Endosc. 2018 August 22; 33(1): p122. |
| [17] | Henneman D, daCosta DW, Vrounracts BC, Van Wagensveld BA, Lagarde SM. Laparoscopic partial cholecystectomy for the difficult gallbladder: a systematic review. Surg Endosc. (2013) 27(2): p351-8. |
| [18] | Zhu YP, Du JD Li WM, Xiao YQ, Xu HB, Zheng F, etal. Gallstone recurrence after successful percutaneous cholecystolithotomy. A 10-year follow up of 439 cases. Hepatobiliary Pancreat Di Int. 2077; 6: p199-203. PMID: 17374582. |
| [19] | De Caluwe D, Akl U, Corbally M. Cholecystectomy versus cholecystolithotomy for cholelithiasis in childhood: long term outcome. J Pediatr Sug. 2001; 36: p1518-21. |
| [20] | Glasgow R, Mulvihill S. Treatment of gall stone disease. In Fildman M, Frideman L, Brandt L (8th Ed.) Sliesenger & Fordtran’s gastrointestinal and liver diseases, Saundry Philadelphia p1419-1437. |
| [21] | Bisgard T, Rosenberg J, Kehlet H from Acute to chronic pain after laparoscopic cholecystectomy: A prospective follow-up analysis. Scand J Gastroenterol 2005; 40: p1358-1364. |
| [22] | Russello D, Di Stefano A, Scala R, Favetta A, Emmi S, Guastella T, etal. Does cholecystectomy always resolve biliary disease? Minerva Chir 1997; 52: p1435-1439. PMID: 9557456. |
| [23] | Anand A, Sharma R, Kapur B, Tandon R. Analysis of symptomatic patients after cholecystectomy: Is the term post-cholecystectomy syndrome and anachromism? Imp Gastroenterol 1995; 52: p1435-1439. PMID: 8644362 |
| [24] | Fugger R Challenging situations in cholecystectomy and strategies to overcome them. Eur Surg. 2021; 53: p106-113. |
| [25] | Eikermann M, Siegel R, Broeders etal. Prevention and treatment of bile duct injuries during laparoscopic cholecystectomy: the clinical practice guidelines of the European Association of Endoscopic Surgery (EAES). Surg Endosc 2012; 26: p3003-3039. |
| [26] | Ellis H. Surgical Case-Histories for the Past. Royal Society of Medicine Press Limited; London, UK: 1994. Chapter 9: Carl Langenbuch. The first cholecystectomy (1882), p57-61. |
| [27] | Sims JM. Cholecystectomy for the removal of gall-stones in dropsy of the gall-bladder. Br. Med. J. 1878; 1: p811-815. |
| [28] | Horiuchi A, Watanbe Y, Doi T, et al. Delayed laparoscopic subtotal cholecystectomy in acute cholecystitis with severe fibrotic adhesions. Sug. Endosc. 2008; 22(12): p2720-2723. |
| [29] | Reynolds W Jr. The first laparoscopic cholecystectomy. JSLS. 2001; 5(1): p89-94. PMID: 11304004; PMCID: PMC3015420. |
| [30] | Henneman D, do Costa DW, Vrouenracts BC, Van Wagensveld BA, Lagarde SM. Laparoscopic partial cholecystectomy for the difficult gallbladder: a systematic review Surg. Endosc. 2003; 17(9): p1437-1439. |
| [31] | Crosthwaite G, McKay C, Anderson JR. Laparoscopic subtotal cholecystectomy. JR Coll Surg. Edinb. 1995; 40(1): p20-21. PMID: 7738890. |
| [32] | Hubert C, Annet L, Van Beers BE, Gigot JF. The ‘inside approach of the gallbladder’ is an alternative to the classic calot’s triangle dissection for a operation in severe cholecystitis. Surg. Endosc. 2010; 24(10): p2626-2632. |
| [33] | Michalowski K, Bornmann PC, Krige JE, Gallagher PJ, Treblanche J. Laparoscopic Subtotal cholecystectomy in patients with complicated acute cholecystitis or fibrosis – J. Surg. 1998; 85(7): p904-906. |
| [34] | Carter DC, Patterson-Brown S. Cholecystectomy, cholecystostomy and exploration of bile duct. In: Carter DC, Russell RCG, Pit HA, Bismuth, eds. Rob & Smith’s Operative Surgery: Hepatobiliary and Pancreatic Surgery; London: Chapman & Hall 1996: p337-50. |
| [35] | King NKK, Priyantha Siriwardana HP, Siriwardena AK. Cholecystitis after cholecystectomy. JR Soc Med. 2002 Mar; 95(3): p138-139. |
| [36] | Ros E, Zambon D. Post cholecystectomy symptoms. A prospective study of gallstone patients before and two years after surgery. Gut 1987; 28: p1500-4. |
| [37] | Bates T, Ebbs SR, Harrison M, A1 Hern RP. Influence of cholecystectomy on symptoms. Br J Surg 1991; 78: p964-7. |
| [38] | Wakabayashi G, Iwashita Y, Hibi T, etal. Tokyo Guidelines 2018: surgical management of acute cholecystitis: safe steps in laparoscopic cholecystectomy for acute cholecystitis. J Hepatobiliary Pancreat Sci. 2018; 25: p73-86. |
| [39] | Kogha A, Suzuki K, O Komura T, Yamashita K, Isogaki J, Kawabe A, Kimuva T. Calculus left in remnant gallbladder cause long-term complications in patients undergoing subtotal cholecystectomy. HPB 2019; 21: p508-14. |
| [40] | C Palanivelu, M. Rangrajan, PA Jategaonkar, MV Madan Kumar, NV Anand. Laparoscopic management of remnant cystic duct calculi: a retrospective study. Ann R Coll. Surg. Engl., 2009 Jan; 91(1): p25-29. |
| [41] | P. Chowbey, V. Soni, A. Sharma, R. Khullar, M Baijal. Residual gall stone disease – Laparoscopic management. Ind J Surg., 2010 Jun; 72(3): p220-225. |
| [42] |
Hamida WB, Jerraya H, Nasseh S, Haloui N, Khalfallan M, Nourea M. The complications of subtotal cholecystectomy: A case report: Int J Surg Case Rep. 2021; 83: 105950.
https://doi.org/10.1016/j.ijscr.2021.105950 Epub 2021 Apr 30 |
| [43] | Strasberg SM, Pucchi MJ, Dezeil, Burnt LM. Subtotal cholecystectomy ‘fenestrating’ vs ‘reconstituting’ subtypes and the prevention of bile duct injury: definitions of the optimal procedure in difficult operative conditions. J Am Coll Surg. 2016; 222(1): p89-96. |
| [44] | Raimandas Lunevicius, Saburo Matsubara. Review Literature on Partial Resections of the Gall Bladder, 1898-2022: The Outline of the Conception of Subtotal Cholecystectomy and a suggestion of Use the Terms ‘Subtotal Open-Tract Cholecystectomy’ and ‘Subtotal Closed-Tract Cholecystectomy’. J Clin Med. 2023 Feb 3; 12(3): p1230. |
| [45] | H. Demetriades, MG Pramate Ftakis, I Kanellos, S Angelopoulus, I Mantzoros, D Betsis. Retained Gallbladder Remnant After Laparoscopic Cholecystectomy. J Laparoendoscopic & Advanced Surgical Techniques. 2008 April 1; 18(2): p276-279. |
| [46] | Madding GF. Subtotal cholecystectomy in acute cholecystitis. Am J Surg. 1955; 89(3): p604-607. |
| [47] | Strasberg SM. A three-step conceptual roadmap for avoiding bile and injury in laparoscopic cholecystectomy: an invited perspective review. J Hepatobeliary Pancreat Sci (2019) 26(4): p123-7. |
| [48] | Ming W, Ying T, Toh J, Shelat VG, Wei C, Sameer H, et al. Subtotal cholecystectomy: early and long-term outcomes. Surg. Endosc 2020; 34: p4536-42. |
| [49] | Tang A, Cohan CM, Beattie G, Mooney CM, Chiang A, Keiley JA. Factors that predict the need for subtotal cholecystectomy. Am Surg. 2021; 87(8): p1245-51. |
| [50] | Toro A, Teodoro M, Khan M, Schembari E, Di Saverio S, Catena F, etal. Subtotal cholecystectomy for difficult acute cholecystitis: how to finalize safety by laparoscopy – a systematic review. World J Emerg Surg. 2021; 16(1): p45. |
| [51] | Boyd K, Bradley NA, Cannings E, Shearer C, Wadhwan H, Wilson MSJ, et al. Laparoscopic subtotal cholecystectomy; change in practice over a 10-year period. HPB 2022; 24(5): p759-63. |
| [52] | Chavez-villa M, Dominguez-rosando I. Subtotal Cholecystectomy after failed critical view of safety is an effective and safe bail out surgery. J. Gastrointest Surg. 2021; 25: p2553-61. |
| [53] | Camilo Ramirez-Giraldo, Andres Torres-Gullar, and Isabella Van-Londono. Sate of the art in subtotal cholecystectomy: An overview. Front Surg. 2023 Apr 21: 10: 1142579. |
| [54] | Schein M, Rogers PN, Assalia A, Lane R. Schein’s Common Sense Emergency Abdominal surgery. Springer 2010; 3: p192. |
| [55] | Di Cataldo A, Avogadro GV, Cannizzaro PD, Latino R. Subtotal Cholecystectomy for difficult gall bladder: a brilliant solution or a lesser skill in biliary surgery? Surgery (2021); 170(3): p989. |
| [56] | Flum DR, Cheadle A, Prela C, etal. Bile duct injury during cholecystectomy and survival in medicare beneficiaries. JAMA 2003; 290: p2168-2173. |
| [57] | Savader SJ, Lillemoe KD, Prescott CA, etal. Laparoscopic cholecystectomy related bile duct injuries: a health and financial disaster. Ann Surg 1997; 225: p268-273. |
| [58] | Moossa AR, Mayer AD, Stabile B. Latrogenic injury to the bile duct who, how, where? Arch Surg. 1990; 125: p1028-1030. |
| [59] | Salky BA, Edye MB. The difficult Cholecystectomy: problems related to concomitant diseases. Semin Laparosc Surg. 1998; 5(2): p107-114. |
| [60] | Laws HL. The difficult cholecystectomy problems during dissection and extraction Semin Laparosc Surg. 1998; 5(2): p81-91. |
| [61] | Kehr H. Introduction to the Differentiated Diagnosis of the Separate forms of Gallstone Disease: Based upon His Own Experiences Gained in 433 Laparotomies for Gallstones. P Blakiston’s Son & Co.; Philadelphia, PA, USA: 1901, p370. |
| [62] | Kehr H. Die Praxis der gallenwage. Chirur in Wort and Bild; 1913, 1080P. |
| [63] | Zhu J, Zhang Z. Laparoscopic remnant cholecystectomy and transcystic common bile duct exploration for gallbladder cystic duct remnant with stones around and cholecholethiasis after cholecystectomy. J. Laparoendo SC Adv. Surg. Tech. 2015; 25: p7-11. |
| [64] | Johnston WR, Flower KJ, Williams GA, Grossman JG, Hammill CW, Hawkins WG, A Diagnosis Reconsidered: The Symptomatic Gallbladder Remnant. J Hepatobiliary Pancreatic Sci. 2019 Apr; 26(4): p137-143. |
| [65] | LM Brunt, DJ Deziel, DA Telem, etal Safe cholecystectomy multi-society practice guideline and stratus-of-the-art consensus on prevention of bile duct injury during cholecystectomy. Surg. Endosc, 2020; 34: p2827-2855. |
| [66] | A Seshadri, AB Peitzman. The difficult cholecystectomy: What you need to know. J Trauma Acute Care Surg, 2024; 97: p325-336. |
| [67] | Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T. Intraoperative Cholangiography and risk of common bile duct injury during cholecystectomy. JAMA 2003; 289: p1639-44. |
| [68] | M Al-Azzawi, M Abouelazyem, C Parmar, R Singhal, B Amar, A Martinino, S D Atici, K Mahawar. A systematic review on laparoscopic subtotal cholecystectomy for difficult gallbladder: a lifesaving bailout or an incomplete operation? Ann R Coll Surg Engl. 2024 Mar; 106(3): 205-212. |
| [69] | Hussain M, Nagral. Biliary pancreatitis secondary to stone from gallbladder remnant. Tropical Gastroenterology 2010; 31: p230-233. |
| [70] | S H Ryou, HJ Kim. Successful removal of remnant cystic duct stump stone using single operator cholangioscopy – guided electrohydraulic therapy: two case reports Clin Endosc, 2023; 56(3): p375-380. |
| [71] | Jebakumar GS, Muthiah J, Jayapal L, Kumar RS, Tasgaon Kar S, Anand KSS, Jamed JKA, Swain SK, Raghunath KJ, Reddy PK, Balachandar TG. Laparoscopic management of remnant gall bladder with stones: Lesson from a tertiary care centre’s experience. Laparoscopic, Endoscopic and Robotic Level I, II or III Subtotal Cholecystectomy Surgery. 2024; 7(1): p27-33. |
| [72] | Chowbey PK, Bandyopadhyay SK, Sharma A, Khullar R, Soni V, Baijal M. Laparoscopic reintervention for residual gallstone disease, Surgical Laparoscopy, Endoscopy and Percutaneous Techniques 2003; 13(1): p31-35. |
| [73] |
Samir O Cawich, Carlos Wilson, Lindberg K Simpson, Akil J Baker. Stump Cholecystitis: Laparoscopic Completion cholecystectomy with basic laparoscopic equipment in a resource. Poor Setting Case Reports in Medicare 2014; 1: 1787631.
https://doi.org/10.1155/2014/787631 . Epub 2014 Aug 21. |
APA Style
Nigam, V. K., Nigam, S. (2025). Nigam's Classification of Subtotal Cholecystectomy According to the Level of Resection (NCSC-LR). International Journal of Gastroenterology, 9(1), 66-76. https://doi.org/10.11648/j.ijg.20250901.21
ACS Style
Nigam, V. K.; Nigam, S. Nigam's Classification of Subtotal Cholecystectomy According to the Level of Resection (NCSC-LR). Int. J. Gastroenterol. 2025, 9(1), 66-76. doi: 10.11648/j.ijg.20250901.21
@article{10.11648/j.ijg.20250901.21,
author = {Vinod Kumar Nigam and Siddharth Nigam},
title = {Nigam's Classification of Subtotal Cholecystectomy According to the Level of Resection (NCSC-LR)
},
journal = {International Journal of Gastroenterology},
volume = {9},
number = {1},
pages = {66-76},
doi = {10.11648/j.ijg.20250901.21},
url = {https://doi.org/10.11648/j.ijg.20250901.21},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20250901.21},
abstract = {Subtotal cholecystectomy is performed in difficult gallbladder where total cholecystectomy is avoided due to risk of bile duct injury and other complications as the structures of Calot’s triangle are difficult to identify due to severe inflammation, fibrosis and dense adhesions. The remnant gallbladder can cause early and late complications such as bile leak, recurrence of stone formation and acute stump cholecystitis. The knowledge of size of remnant gallbladder in advance can help in diagnosis and decision making for handling the remnant gallbladder complications. Nigam’s Classification of Subtotal Cholecystectomy according to the Level of Resection (NCSC-LR) plays an important role in such situations and helps the treating surgeon in diagnosis and treatment of post subtotal cholecystectomy complications by knowing the level of resection (size of remnant gallbladder) as per previous operation notes.
},
year = {2025}
}
TY - JOUR T1 - Nigam's Classification of Subtotal Cholecystectomy According to the Level of Resection (NCSC-LR) AU - Vinod Kumar Nigam AU - Siddharth Nigam Y1 - 2025/06/30 PY - 2025 N1 - https://doi.org/10.11648/j.ijg.20250901.21 DO - 10.11648/j.ijg.20250901.21 T2 - International Journal of Gastroenterology JF - International Journal of Gastroenterology JO - International Journal of Gastroenterology SP - 66 EP - 76 PB - Science Publishing Group SN - 2640-169X UR - https://doi.org/10.11648/j.ijg.20250901.21 AB - Subtotal cholecystectomy is performed in difficult gallbladder where total cholecystectomy is avoided due to risk of bile duct injury and other complications as the structures of Calot’s triangle are difficult to identify due to severe inflammation, fibrosis and dense adhesions. The remnant gallbladder can cause early and late complications such as bile leak, recurrence of stone formation and acute stump cholecystitis. The knowledge of size of remnant gallbladder in advance can help in diagnosis and decision making for handling the remnant gallbladder complications. Nigam’s Classification of Subtotal Cholecystectomy according to the Level of Resection (NCSC-LR) plays an important role in such situations and helps the treating surgeon in diagnosis and treatment of post subtotal cholecystectomy complications by knowing the level of resection (size of remnant gallbladder) as per previous operation notes. VL - 9 IS - 1 ER -
General and Minimal Access Surgery, Max Hospital, Gurgaon, India
General and Minimal Access Surgery, Max Hospital, Gurgaon, India